In the 1950s, America saw the beginning of “car culture,” and today there are roughly 210 million licensed drivers in the United States. Driving is almost second-nature. However, if you’re used to driving a Volvo and I give you the keys to a Mercedes, it may take a moment or two of adjustments before you’re ready to cruise down the highway. It’s not because you don’t know how to drive; it’s just a matter of learning a new system.
A cone beam computed tomography (CBCT) system is not unlike becoming comfortable with a different make and model of car. I’ve been operating my system for years now, and can comfortably “turn on a dime” or “shift gears.” However, when I invite a referring doctor to “go for a drive,” e.g., share the 3D imaging software for collaborative cases or email a screenshot of a scan, there may be a bit of a learning curve. But once the general practitioner learns to properly view the scans, it not only helps me build stronger relationships with them but allows for me to gain greater future referrals.
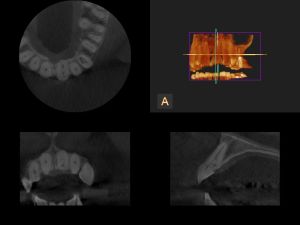 First, CBCT allows me to view a patient’s anatomy in stunning 3D detail and can reveal much more than what a traditional panoramic X-ray could. I share these CBCT scans with the referring doctor and usually get one of two responses—“Yes, good, proceed with treatment,” or “Your system showed you all that?! Tell me more…” Of course, it’s perfectly acceptable for the referring doctor to trust my judgment and go with my proposed treatment. However, there’s something to be said about the GP who wants to gain a better understanding of the CBCT findings. Also, greater communication increases the chances that future treatment will have fewer hurdles.
First, CBCT allows me to view a patient’s anatomy in stunning 3D detail and can reveal much more than what a traditional panoramic X-ray could. I share these CBCT scans with the referring doctor and usually get one of two responses—“Yes, good, proceed with treatment,” or “Your system showed you all that?! Tell me more…” Of course, it’s perfectly acceptable for the referring doctor to trust my judgment and go with my proposed treatment. However, there’s something to be said about the GP who wants to gain a better understanding of the CBCT findings. Also, greater communication increases the chances that future treatment will have fewer hurdles.
So if that’s the case, I take the time to meet with the general practitioner in person to go over the scan in more detail. For example, a CBCT can elucidate a proposed implant site with a buccal-lingual cross cross-sections for both horizontal measurements and for visualizing the distance from the crestal bone to the nerve canal. My 3D imaging software is also easy to share, which gives the GP a bit more freedom to play around in the scan and take the CBCT for a “test drive.”
When the general practitioner has confidence in my CBCT system and my own capabilities, it can also help them put their patients’ mind at ease. Essentially—“Don’t worry, I’m sending you to the best. They have the most advanced technology to get to the root of this problem.” CBCT, therefore, plays a vital role in enhancing communication with the referring doctor. For example, if a GP has a patient with multiple failed root canals CBCT may reveal the missed canals. I can share a screenshot in an email, or as part of a report, and show, for example, a missed MB2 and offer treatment recommendations.
Referrals are glad they partnered with me because of my CBCT system. I’m always happy to invite GPs to “go for a ride” in my CBCT system; it makes them more knowledgeable and also more likely to send referrals my way. Most importantly, it helps our patients receive the best treatment available today.
| Our Family of Brands | ||
 |
 |
|
© 2024 Carestream Dental LLC. All Rights Reserved